EHR-FHIR integration for payer data exchange follows Da Vinci patterns. Understanding what ships in production shapes realistic expectations.
Data flows in production
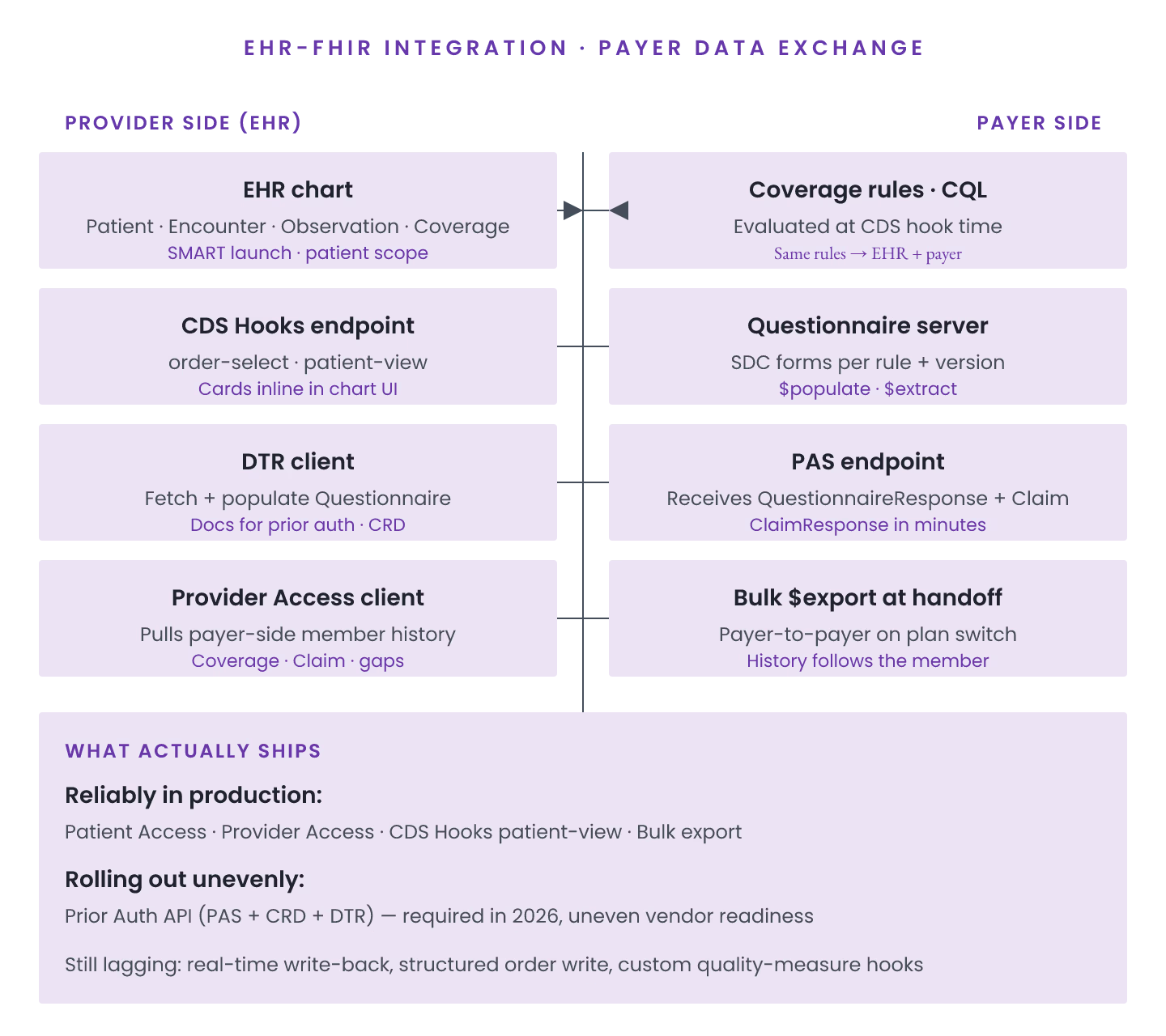
1. Provider → Payer. Prior authorization via Da Vinci PAS; claims via X12 837. 2. Payer → Provider. Da Vinci PDex Provider Access delivers coverage, clinical data. 3. Payer → Patient. Patient Access API exposes member data. 4. Payer → Payer. Cross-payer member data via Bulk Data IG.
CMS-0057 timeline
| API | Mandate |
|---|---|
| Patient Access | Live 2024 |
| Provider Access | Live 2024 |
| Payer-to-Payer | Live 2025 |
| Prior Authorization | Rolling 2026-2027 |
FHIR resources involved
1. **Patient — Member identity. 2. Coverage — Insurance coverage. 3. ExplanationOfBenefit — Claims adjudication. 4. Claim — Claims data. 5. Condition, Observation, MedicationRequest** — Clinical data.
Common integration challenges
1. Terminology binding differences. 2. MPI federation across payer + provider. 3. Auth model coordination. 4. Rate limiting for provider queries. 5. Consent tracking.
Vendor state (mid-2026)
| Solution | PDex | PAS | Bulk Data | SMART BE |
|---|---|---|---|---|
| Cognizant | Full | Full | Full | Full |
| Availity | Full | Full | Full | Full |
| Change Healthcare | Full | Full | Full | Full |
| Custom | Configurable | Manual | Configurable | Configurable |
Integration surface
1. FHIR REST endpoints per API. 2. SMART Backend Services for auth. 3. Bulk data storage. 4. Terminology server. 5. Audit trail.
Common EHR-payer integration mistakes
1. Custom auth vs. SMART BE. 2. Manual data mapping vs. Da Vinci profiles. 3. Sync-only bulk export. 4. Missing race/ethnicity extensions. 5. Aggressive rate limits.
EHR-FHIR integration for payer data exchange is CMS-mandated in 2026. Da Vinci profiles + SMART auth are the shipping path; custom is legacy.