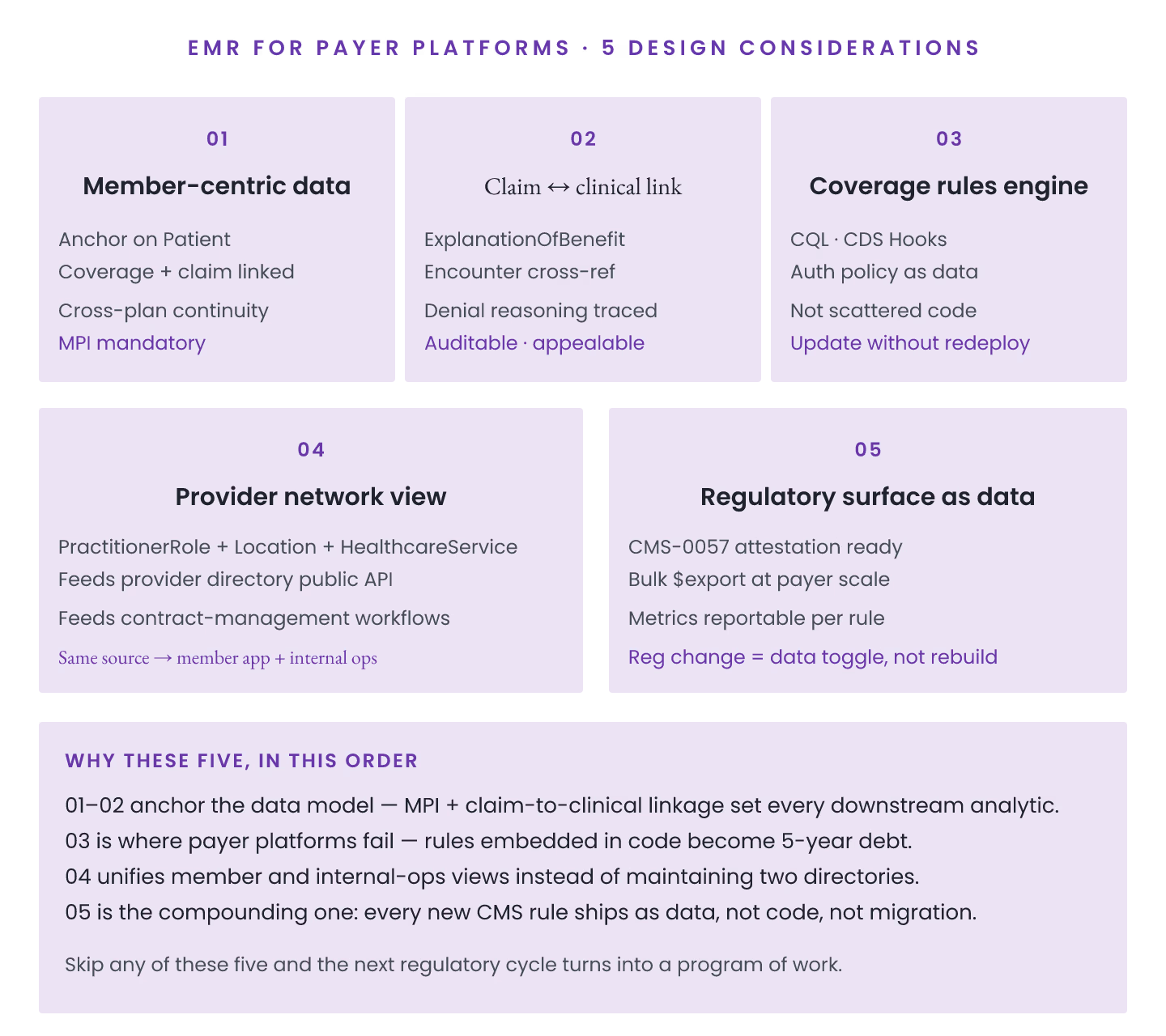
Payer-side EMR-adjacent platforms have distinct design considerations. Five that shape payer-platform architectures.
Consideration 1: Coverage data as primary resource. Coverage resource is central for payers, unlike provider-side where Patient dominates. Design around Coverage lifecycle.
**Consideration 2: ExplanationOfBenefit at scale.** Payers generate massive EOB volumes (10s of millions monthly). Bulk-data-first architecture.
Consideration 3: Cross-payer member reconciliation. Members switching between payers. MPI federation across systems.
Consideration 4: Prior authorization workflow. Da Vinci PAS profiles. Complex approval logic.
Consideration 5: Payer-specific terminology. ClaimResponse codes, ExplanationOfBenefit adjudication codes. Beyond standard SNOMED/LOINC.
Investment areas
1. Bulk data pipeline (very high volume). 2. MPI infrastructure for cross-payer. 3. Da Vinci profile implementation. 4. Payer-specific terminology. 5. Prior authorization workflow engine.
Common payer-side mistakes
1. Provider-side thinking applied to payer. 2. Missing bulk data infrastructure. 3. Weak MPI federation. 4. Custom PA workflow instead of Da Vinci PAS. 5. Terminology binding drift.
Volume characteristics
| Data type | Typical volume |
|---|---|
| Coverage records | 100k-10M members |
| EOB records | 1M-100M per month |
| Prior auth requests | 10k-1M per month |
| Member enrollment | Continuous |
Vendor state (mid-2026)
| Solution | Payer focus | CMS-0057 compliance |
|---|---|---|
| Cognizant | Enterprise payer | Full |
| Availity | Payer integration | Full |
| Custom on Aidbox | Configurable | Custom |
| Custom on HAPI | Configurable | Custom |
Data quality prerequisites
1. $validate pass rate >97%. 2. Reference integrity >99%. 3. Terminology binding compliance >98%. 4. Duplicate rate <2%.
Payer-side platforms are a distinct FHIR use case. Understanding the five considerations above shapes reliable delivery.